
Translate this page into:
A comparative study of proximal femoral nail and dynamic hip screw for intertrochanteric fractures of the femur
*Corresponding author: Aabid Husain Ansari, Department of Orthopaedics, Pacific Institute of Medical Science, Udaipur, Rajasthan, India. draabidhusainansari@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Ansari AH, Ansari AH. A comparative study of proximal femoral nail and dynamic hip screw for intertrochanteric fractures of the femur. Karnataka Med J. 2024;47:3-8. doi: 10.25259/KMJ_13_2024
Abstract
Introduction:
Intertrochanteric fracture is one of the most common fractures of the hip. However, the implant of choice for type II intertrochanteric fracture is still under debate. The aim of this study was to compare the functional outcomes of proximal femoral nail (PFN) and dynamic hip screw (DHS) in treatment of intertrochanteric fractures.
Material and Methods:
We did a prospective comparative study on 60 patients of type II intertrochanteric fractures operated with closed/open reduction and internal fixation with either DHS or PFN between October 2018 and March 2023. During each follow-up, the functional outcome of patients was calculated using the Harris hip score.
Results:
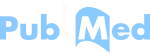
There was a statistically significant difference present in average functional scores between the two groups at 1 month, 3 months and 6 months; however, no difference was seen at the end of 12th month follow-up. Functional outcomes in the DHS group were excellent in 34.78%, fair in 17.39%, good in 43.48% and poor in 4.35%. In the PFN group, results were excellent in 56.52%, fair in 8.70% and good in 34.78% and no poor results were seen.
Conclusion:
In stable two-part intertrochanteric femur fractures, both PFN and DHS are equally effective but due to minimal invasiveness. PFN is a better implant of choice than DHS in the treatment of elderly patients with intertrochanteric fractures.
Keywords
Dynamic hip screw
Proximal femoral nail
Intertrochanteric fractures
Harris hip score
INTRODUCTION
Intertrochanteric fracture is one of the most common fractures of the hip, especially in the elderly with osteoporotic bones.[1] The treatment goal of these fractures is stable fixation, which allows early mobilisation of the patient and reduces the associated morbidity and mortality. The conservative treatment has a high complication rate,such as decubitus ulcers, urinary tract infection, joint contractures, pneumonia, thromboembolism, varus deformity and shortening of limb. Hence, conservative treatment should only be considered in non-ambulatory patients, patients with terminal diseases with <6 weeks of life expectancy, surgically unfit patients, and active infectious diseases.[2] The surgical treatment of intertrochanteric fractures has evolved since the usage of the fixed nail plate, dynamic hip screws (DHSs), modified DHS and intramedullary devices. The advantages and disadvantages of the DHS have been well established in several studies done in the past.[3] However, many studies compare the DHS with Gamma nail.[4-6] There are limited studies that studies compare the DHS with proximal femoral nail (PFN), which is being preferred by many.
This study was conducted to compare the functional and radiological outcome of PFN with DHS in the treatment of intertrochanteric fractures.
AIMS AND OBJECTIVES
To compare the functional and radiological outcome of PFN with DHS in the treatment of intertrochanteric fractures.
MATERIAL AND METHODS
We conducted a prospective comparative study from October 2018 to March 2023 on patients with type II intertrochanteric fractures operated with closed/open reduction and internal fixation with either DHS or PFN [Figures 1 and 2]. A total of 60 patients have been included, out of which 30 belonged to group 1 and were operated with PFN, and the rest 30 were to group 2, operated with DHS. Informed consent was obtained from each patient. We included the surgically fit patients with age more than 50 years of age who have been diagnosed as having type II intertrochanteric fractures. Polytrauma patients, patients with compound fractures or pathological fractures or concomitant shaft femur fractures, patients unfit for the surgery and admitted for re-operation were excluded from the study. The fracture was classified using association of osteosynthesis (AO) classification. Implant, either DHS or PFN was randomly selected. For DHS, the length of Richard’s screw was measured preoperatively on antero-posterior (AP) view X-ray subtracting magnification. The neck shaft angle was measured using a goniometer on AP view X-ray on the unaffected side to determine the angle for the barrel plate. At least four holes and a length side plate, was used. PFN Nail diameter was determined by sequential reaming of the femoral canal. A standard length PFN (180 mm or 240 mm) and 135° angle were used in all our cases. All patients were operated on a fracture table under spinal anaesthesia by a single operating surgeon. First, closed reduction was tried for all the patients and open reduction was done only for fractures which were not reduced by closed reduction. Antibiotics were administered 30 min before incision and continued for 48 h postoperatively. Immediate post-operative hip X-ray was taken to ascertain the fracture reduction and position of the implant. Physiotherapy was started from day 1, static quadriceps, knee and ankle mobilisation exercises were started and all patients were allowed to be weight-bearing as tolerated. Wound inspection and drain removal was done on day 2. Most of the patients were discharged on the 5th or 6th post-operative day. Stitches were removed on the 14th day. All patients were followed up at 1 month, 3 months, 6 months, and 12 months after the surgery. At each follow-up, pain, ambulatory status, and functional outcome of patients using Harriship score (HHS) were evaluated, and hip X-rays were taken to check the status of fracture union. The HHS includes pain, function of joint, deformity and range of movements. The HHS score gives a maximum of 100 points. The higher the HHS, the less the dysfunction. HHS <70 is considered a poor result; 70–80 is fair, 80–90 is good and 90–100 is excellent.

- A 72-year-old female patient with intertrochanteric fracture fixed with proximal femur nail. (a) Pre-operative radiograph. (b) Immediate post-operative radiograph.

- A 68-year-old male patient with intertrochanteric fracture fixed with dynamic hip screw. (a) Pre-operative radiograph. (b) Immediate post-operative radiograph.
Statistical analysis was performed with the Statistical Package for the Social Sciences (SPSS) version 19.0 (SPSS Inc./IBM, Chicago, IL). P < 0.05 was considered to be statistically significant.
RESULTS
A total of 60 patients were included in the study. The average age was 60 years (range: 66–86 years). In our study, the most common mode of injury was trivial trauma (77%). The patient characteristics of both groups were not significantly different [Table 1].
| Group I (PFN) | Group II (DHS) | |
|---|---|---|
| Number of patients | 30 | 30 |
| Mean patients age (Y) | 60.25 | 62 |
| Gender (Male/Female) | 16/14 | 17/13 |
| Side (Right/Left) | 20/10 | 18/12 |
PFN: Proximal femoral nail; DHS: Dynamic hip screw
The average intraoperative blood loss was greater in DHS group (220 mL vs. 80 mL, P = 0.01). Five out of 30 patients in the DHS group required blood transfusion postoperatively. The mean surgery duration was also more in DHS group (62 min vs. 45 min, P = 0.02). In PFN, incision was smaller and duration of surgery was shorter so there was less tissue damage and hence lesser blood loss.
The average sliding in the PFN group was 4.3 mm as compared to 6.9 mm in the DHS group (P = 0.001). The average limb shortening in DHS group was 9.33 mm as compared with PFN group, which was only 4.72 mm (P = 0.02). Even though there was more shortening in the DHS group, it was not significant enough to cause any gait or functional impairment. The average hospital stay was 8.24 days (5–9 days) in case of DHS while 7.35 days (4–8 days) in the case of PFN (P = 0.001). Return to pre-injury walking ability in the DHS group was on an average of 12 weeks compared to PFN, which was 8 weeks (P = 0.03). The average tip-apex-distance in the DHS group was 18.3 mm (range 12–24 mm). As PFN is an intramedullary load-sharing device as compared to DHS, which is a load-bearing device, full and partial weight-bearing was started at an early stage for PFN patients [Table 2]. The mean time for radiological signs of the union was almost the same in both groups (3 ± 1 months).
| Group I (PFN) | Group II (DHS) | P-value | |
|---|---|---|---|
| Average length of incision (cm) | 4.2 cm | 15 cm | <0.05 |
| Average intraoperative blood loss (mL) | 80+16.40 mL | 220+44.98 mL | 0.01 |
| Radiation exposure | 40+1.6 (in no.) | 20+4 (in no.) | <0.05 |
| Mean operative time (minutes) | 45+18 min | 62+3.2 min | 0.02 |
| Average hospital stay (days) | 7.35 days | 8.24 days | 0.001 |
| Sliding | 4.3 mm | 6.9 mm | 0.001 |
| Shortening | 4.72 mm | 9.3 mm | 0.02 |
| Implant failure | 1 | 2 | <0.05 |
| Non-union | 0 | 1 | <0.05 |
| Deaths | 1 | 1 | >0.05 |
| Infection | 0 | 2 | <0.05 |
| Greater trochanter splintering | 2 | 0 | >0.05 |
| Revision surgery | 1 | 3 | >0.05 |
PFN: Proximal femur nail, DHS: Dynamic hip screw
Total 3 patients developed implant failure (1 in PFN group and 2 in DHS group) and revision surgery was done. In PFN group, “Z” pattern of implant failure was the reason, whereas in DHS group, the implant failed due to a lag screw cut out. In the DHS group, one patient developed non-union, which was due to jamming, and was treated with bone grafting. In the PFN group, a greater trochanter was splintered intraoperatively in two patients, which was fixed by tension band wiring. Two patients developed superficial surgical site infection in the DHS group, which was managed by regular dressing and appropriate antibiotics. There was one death each in both groups after 3–4 months of surgery due to medical comorbidities.
There was a statistically significant difference present in average functional scores calculated using the HHS between two group at 1 month (33.33 and 25.25, respectively), 3 months (54.85 and 346.65, respectively) and 6 months (85.20 and 68.25, respectively); however, this difference disappeared at the end of 12th-month follow-up with both scores being almost the same (90.33 and 89.55, respectively).
DISCUSSION
Hip fractures are significantly associated with higher mortality and morbidity rate.[7] In the past few decades, various treatment methods of intertrochanteric fractures have evolved. The treatment still merits the type of fracture, quality of bone, and condition of the patient. In 1960, DHS was developed for the fixation of intertrochanteric fractures. [8-10] DHS allowed controlled compressive collapse at the fracture site without complications of screw cut out and implant breakage associated with a nail plate. However, the extensive surgical dissection, more intraoperative blood loss and more operative time required for this procedure often made it a contraindication in the elderly with comorbidities. DHS also failed to achieve good results in extremely unstable and reverse oblique fracture.[8-10] In 1997, intramedullary device (PFN) was introduced for fixation of intertrochanteric fractures. It was designed to overcome implant-related complications and facilitate the surgical treatment of unstable intertrochanteric fractures.[11-14] PFN inserted by a minimally invasive procedure, which allows to minimise soft-tissue dissection, thereby reducing surgical trauma and blood loss. The results of our study also demonstrate that operative time, intraoperative blood loss and length of incision in the PFN group are significantly less than in the DHS group.
Pajarinen et al. noted that PFN allows faster post-operative restoration of walking ability when compared to DHS.[2] In our study, patients treated with PFN returned to pre-injury walking status earlier than patients who underwent DHS. PFN creates a shorter lever arm, which translates to a lower bending moment and a decreased rate of mechanical failure.[12] We found PFN to be more useful in unstable and reverse oblique fracture patterns because it is a load-shearing device so it provides better axial telescoping and rotational stability compared to DHS.[15-17] PFN also has biomechanically more stronger than DHS because they can withstand higher static and several-fold higher cyclical loading, so the fracture heals without the primary restoration of the medial support. Due to intramedullary implant, PFN is also acts as a buttress in preventing the medialisation of the shaft.[18,19] Herman et al. suggested that in PFN placing of lag screw within the ‘safe zone’ (second quarter of the head-neck interface line) could significantly reduce the mechanical failure rate.[20] There was no significant difference in the mean HHS between the two groups at 12th month follow-up. In this study, the functional outcome in the DHS group was excellent in 34.78%, fair in 17.39%, good in 43.48% and poor in 4.35%. In PFN group, results were excellent in 56.52%, fair in 8.70% and good in 34.78% and no poor results were seen [Tables 3-5, Figure 3].
| Follow-up | PFN | DHS |
|---|---|---|
| 1 Month | 33.33 | 25.25 |
| 3 Months | 54.85 | 34.65 |
| 6 Months | 85.20 | 68.25 |
| 12 Months | 90.33 | 89.55 |
PFN: Proximal femur nail, DHS: Dynamic hip screw
| Mean HHS | ||
|---|---|---|
| PFN | DHS | |
| Present study | 90.33 | 89.55 |
| Bakshi et al.[21] | 84.4 | 83.75 |
| Qidwai et al.[22] | 83.5 | 73.73 |
| Sharma et al.[23] | 82.2 | 88.7 |
PFN: Proximal femur nail, DHS: Dynamic hip screw, HHS: Harris hip score
| Functional outcome | Present study | Parikh et al.[24] | Harish et al.[25] | Gill et al.[26] | ||||
|---|---|---|---|---|---|---|---|---|
| PFN | DHS | PFN | DHS | PFN | DHS | PFN | DHS | |
| Excellent | 56.52 | 34.78 | 15 | 23 | 72.73 | 50 | 20 | 15 |
| Good | 34.78 | 43.48 | 54 | 19 | 9.1 | 13.33 | 75 | 35 |
| Fair | 8.70 | 17.39 | 27 | 50 | 9.1 | 13.33 | 5 | 30 |
| Poor | 0 | 4.35 | 4 | 8 | 9.1 | 13.33 | 0 | 20 |
PFN: Proximal femur nail, DHS: Dynamic hip screw
- Bar diagram showing the functional outcome of the dynamic hip screw and the proximal femur nail group based on Harris hip score. PFN: Proximal femur nail, DHS: Dynamic hip screw
In the present study, two patients developed superficial surgical site infection in the DHS group which was managed by regular dressing and appropriate antibiotics. Patients treated with DHS have a high incidence of superficial infection due to lengthier incisions.[21-26] Three patients (two patients in the DHS group and one patient in the PFN group) developed limb length discrepancy of up to 1–2 cm, which is also similar to the study conducted by Bakshi et al.[21] The limitations of this study include a small sample size and small follow-up.
CONCLUSION
In stable two-part intertrochanteric femur fractures, both PFN and DHS are equally effective but due to minimal invasiveness PFN is a better implant of choice than DHS in the treatment of elderly patients with intertrochanteric fracture.
Ethical approval
The research/study approved by the Institutional Review Board at Pacific Institute of Medical Science, number STU/PIMS/20284-620-23, dated 15 October 2018.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Unstable intertrochanteric fractures of the hip. J Bone Joint Surg Am. 1967;49:440-50.
- [CrossRef] [Google Scholar]
- Pertrochanteric femoral fractures treated with a dynamic hip screw or a proximal femoral nail: A randomised study comparing post-operative rehabilitation. J Bone Joint Surg Br. 2005;87:76-81.
- [CrossRef] [PubMed] [Google Scholar]
- The treatment of trochanteric fractures of the femur. J Bone Joint Surg Br. 1949;31:190-203.
- [CrossRef] [Google Scholar]
- Fixation of intertrochanteric fractures of the femur. A randomised prospective comparison of the gamma nail and the dynamic hip screw. J Bone Joint Surg Br. 1991;73:330-4.
- [CrossRef] [PubMed] [Google Scholar]
- A prospective randomised comparison of the dynamic hip screw and the gamma locking nail. J Bone Joint Surg Br. 1993;75:789-93.
- [CrossRef] [PubMed] [Google Scholar]
- Fixation of intertrochanteric hip fractures: Gamma nail versus dynamic hip screw. A randomized, prospective study. Can J Surg. 1995;38:516-20.
- [Google Scholar]
- Worldwide projection for hip fracture. Osteoporos Int. 1997;7:407-13.
- [CrossRef] [PubMed] [Google Scholar]
- Femoral neck fractures [Abridged] a new method of treatment of pertrochanteric fractures. 1970:1120-1121.
- [CrossRef] [Google Scholar]
- Treatment of fragments, loss of bony substance and pseudarthrosis of femur and tibia using screw fixation (40 cases) Rev Chir Orthop Reparatrice Appar Mot. 1978;64:33-5.
- [Google Scholar]
- Fractures of hip and pelvis In: Campbell's operative orthopaedics. Netherlands: Elsevier; 1992.
- [Google Scholar]
- The AO/ASIF-proximal femoral nail (PFN): A new device for the treatment of unstable proximal femoral fractures. Injury. 1999;30:327-32.
- [CrossRef] [PubMed] [Google Scholar]
- Use of an intramedullary hip-screw compared with a compression hip-screw with a plate for intertrochanteric femoral fractures. A prospective, randomized study of one hundred patients. JBJS. 1998;80:618-30.
- [CrossRef] [PubMed] [Google Scholar]
- Fatigue failure of sliding hip screw in hip fractures a report of three cases. J Orthop Trauma. 1991;3:325-31.
- [CrossRef] [PubMed] [Google Scholar]
- Gamma nails and dynamic hip screws for pertrochanteric fractures. A randomized prospective study in elderly patients. J Bone Joint Surg Br. 1992;74:345-51.
- [CrossRef] [PubMed] [Google Scholar]
- Biomechanical analysis of the sliding characteristics of compression hip screws. J Bone Joint Surg Am. 1980;62:1308-14.
- [CrossRef] [PubMed] [Google Scholar]
- Classification and treatment of intertrochanteric fractures. Arch Surg. 1949;58:853-66.
- [CrossRef] [PubMed] [Google Scholar]
- Trochanteric fractures treated with McLaughlin plate. Acta Ortho Scand. 1975;46:795-803.
- [CrossRef] [PubMed] [Google Scholar]
- The proximal femoral nail (PFN)-a minimal invasive treatment of unstable proximal femoral fractures: A prospective study of 55 patients with a follow-up of 15 months. Acta Orthop Scand. 2003;74:53-8.
- [CrossRef] [PubMed] [Google Scholar]
- Stabilisation of unstable trochanteric femoral fractures. Dynamic hip screw (DHS) with trochanteric stabilisation plate vs. proximal femur nail (PFN) Vergleichzwischen PFN und DHS mitTrochanterabstützplatte. Der Unfallchirurg. 2003;106:39-47.
- [CrossRef] [PubMed] [Google Scholar]
- Radiological evaluation of intertrochanteric fracture fixation by the proximal femoral nail. Injury. 2012;43:856-63.
- [CrossRef] [PubMed] [Google Scholar]
- Comparative study between DHS and PFN in intertrochanteric fractures of femur. Int J Orthop Sci. 2018;4:259-62.
- [CrossRef] [Google Scholar]
- Comparative study of functional outcome of the intertrochanteric fracture of femur managed by dynamic hip screw and proximal femoral nail. Natl J Clin Orthop. 2019;3:26-30.
- [CrossRef] [Google Scholar]
- Treatment of stable intertrochanteric fractures of the femur with proximal femoral nail versus dynamic hip screw: A comparative study. Rev Brasil Ortop. 2018;53:477-81.
- [CrossRef] [Google Scholar]
- Functional and radiological outcome of proximal femoral nailing versus dynamic hip screw in unstable intertrochanteric femur fractures. Int J Res Orthop. 2018;4:861.
- [CrossRef] [Google Scholar]
- A comparative study between DHS and PFN for the treatment of IT fractures. Nat J Clin Orthop. 2019;3:1-7.
- [CrossRef] [Google Scholar]
- Dynamic hip screw with locked plate VRS proximal femoral nail for the management of intertrochanteric fracture: A comparative study. Int J Orthop Sci. 2017;3:173-80.
- [CrossRef] [Google Scholar]




