
Translate this page into:
Rare case of assault with knife penetrating base of the skull – Retrieval and management
*Corresponding author: Kumar Saket, Department of Maxillofacial Surgery, Rajiv Gandhi University of Health Sciences, Bengaluru, Karnataka, India. saket0410@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Vijapur M, Saket K, Kumari K, Kattimani V. Rare case of assault with knife penetrating base of the skull – Retrieval and management. Karnataka Med J. 2024;47:39-42. doi: 10.25259/KMJ_8_2024
Abstract
Addressing a penetrating injury in the maxillofacial region poses significant challenges for oral and maxillofacial surgeons due to the presence or critical structures. Damage to these structures can lead to varying degrees of impairment and a decreased quality of life for the patient. A 48-year-old individual sustained a stabbing injury to the left side of their face. The knife remained lodged inside for 7 h until they were admitted to the trauma unit. The assailant had unsuccessfully attempted to remove the weapon by bending its handle. Following thorough examinations to pinpoint the exact location of the knife, it was safely removed under sedation. The patient experienced successful healing without major complications. The minimisation of scar tissue was achieved through proper debridement and layered linear wound closure. Subsequently, the patient was transferred to the general ward for monitoring and prescribed antibiotics to prevent wound infection. This report includes a detailed account of the weapon retrieval process and its management, along with a review of relevant literature Reconstruction of complicated facial wounds is difficult for surgeons, and early treatment is necessary to avoid additional harm.
Keywords
Trauma
Penetrating injury
Foreign body
Buccal cheek
Attack
INTRODUCTION
Punctate and incised wounds result from the penetration or cutting action of sharp objects, such as knives, which breach the skin or mucous membranes. Foreign objects can become embedded in the body, causing penetrating injuries with potentially serious consequences.[1] However, facial penetrating injuries tend to be less severe compared to those in other body areas, largely due to the face’s innate reflexes that help deflect incoming objects, as well as its smaller surface area.
The facial structure, including robust pillars, buttresses and air-filled spaces in the skull, is adept at absorbing impact, which may mitigate the extent of injury.[2] Fatal facial penetrating injuries are uncommon and typically involve deep structures within the skull. This case report outlines the management of such an injury, which can pose challenges for oral and maxillofacial surgeons due to factors such as the size of the foreign object and limited access. Locating and removing the foreign body is a crucial step, often necessitating imaging studies such as X-rays, computed tomography (CT) scans, magnetic resonance imaging or ultrasound to determine its precise location and composition.[3]
Literature review
According to Sastay et al. (1995), the lodgement of foreign bodies in an area such as the infratemporal fossa is quite rare and only a few cases have been reported in the literature so far.[4]
Wulkan et al. (2005) also report complications associated with foreign body removal due to its critical structures – excessive haemorrhage, infection, pain, swelling and trismus.[5]
CASE REPORT
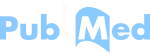
A 48-year-old individual presented to the trauma unit at Karnataka Institute of Medical Sciences, Hubli, reporting a knife stab wound on the left cheek [Figure 1]. The incident had occurred 7 h before they arrived at the trauma department. They mentioned attempting unsuccessfully to remove the weapon by twisting the knife handle. During the extraoral examination, a knife was observed protruding from the patient’s left cheek [Figure 2]. There was no active bleeding, and the patient’s vision remained unaffected. The initial clinical assessment indicated no injury to the cranial area or nearby critical structures, and there was no evidence of bone penetration. The knife blade had penetrated the left buccal cheek region. Before surgery, a CT scan of the brain and mandible was conducted to precisely locate the position of the weapon. The scan revealed that the knife blade had penetrated the floor of the left orbit, traversed the roof of the maxillary sinus and entered the pterygoid fossa [Figure 3]. However, there was no compromise to the base of the skull.

- Clinical pre-operative aspect.

- Opening mouth limitation to 1 finger.
- (a and b) Computed tomography screen with mandibular impression.
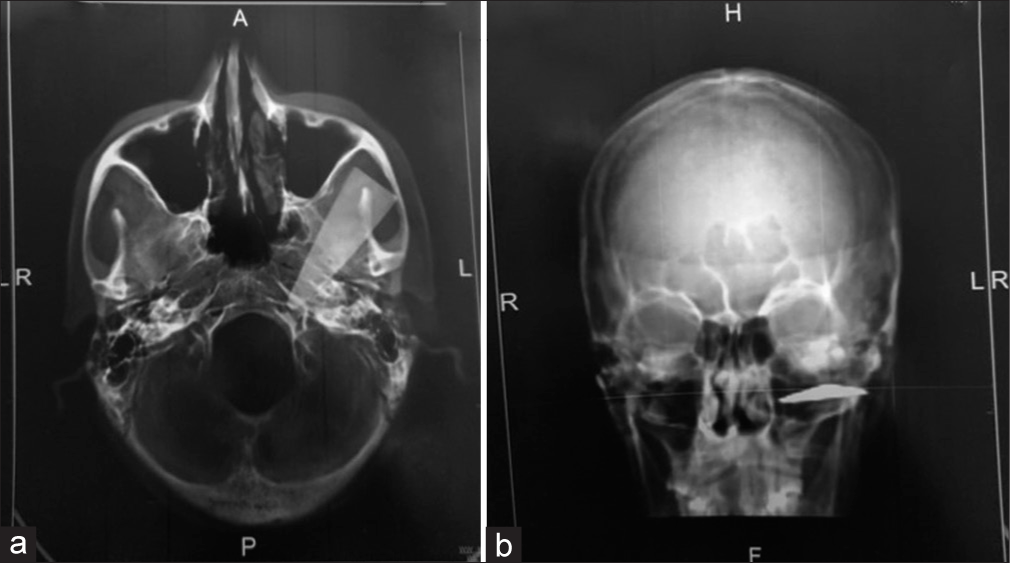
The patient was scheduled for surgery in the operating theatre to remove the knife fragment and close the wound. Under general anaesthesia, a degloving incision was made using an existing laceration in the zygomatic area. The periosteum and muscles were carefully separated, and the arteries were meticulously inspected and protected [Figure 4].
- Wound debrided and cleaned with copious irrigation of iodine and saline.
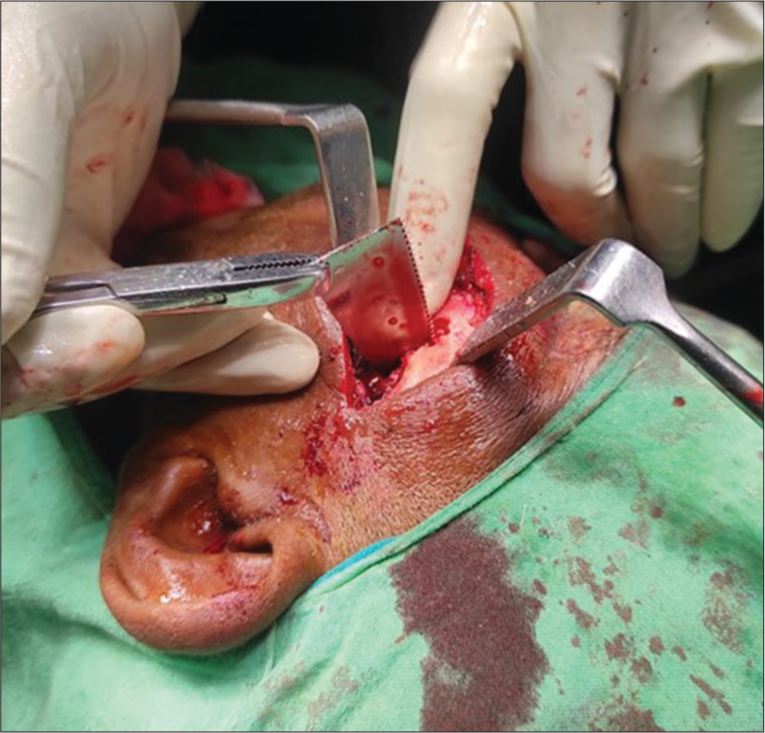
A periosteal elevator was employed to carefully separate the knife fragment from the surrounding soft tissues, creating a pathway for its removal [Figure 5]. Minimal bleeding was observed from the injured area during and after the extraction of the knife piece. Haemostasis was successfully achieved postoperatively. Following the removal of the knife, the patient was orally intubated. The penetrating wound was meticulously inspected, revealing a 7 cm deep laceration on the left side of the face. Fortunately, critical structures such as the orbit, parotid gland with duct and infraorbital nerve were unaffected. To ensure complete removal of any foreign bodies or metal remnants from the wound, thorough irrigation with normal saline and iodine was performed. After surgery, the patient received standard antibiotic treatment with IV augmentin 1.2 mg for 3 days, followed by oral tablets. Pain relief was managed with augmentin 625 mg and diclofenac for the subsequent 5 days. The post-operative recovery was uneventful, with the patient reporting no concerns during the 1-day follow-up evaluation. Sutures remained intact, and there was no evidence of active bleeding. At the 4-month follow-up, a small scar was observed on the left cheek, and the patient reported no ongoing issues or complaints [Figure 6].
- Foreign body removal.

- Post-operative picture (after 4 months).
DISCUSSION
Penetrating knife wounds are a common occurrence, necessitating a comprehensive clinical assessment of facial injuries. The cheek is frequently affected, with critical structures such as the facial nerve, parotid gland and parotid duct being of particular concern (Schultz and Oldham, 1977).[6] In addition, consideration should be given to associated vascular damage, as indicated by signs such as active bleeding, an expanding haematoma, a bruit or a pulse deficit in the superficial temporal artery, all suggestive of penetrating vascular trauma.
CONCLUSION
Reconstructing major facial wounds presents surgeons with several challenges. Balancing aesthetic and functional outcomes is paramount, with no standardised therapeutic protocols in place. Delayed treatment can lead to complications such as infection and necrotising fasciitis, whereas acute injury to the vascular supply may result in full-thickness necrosis of the flap.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- Peterson’s principles of oral and maxillofacial surgery USA: People’s Medical Publishing House; 2012. p. :2000.
- [Google Scholar]
- Fascial space infections In: Bonanthaya K, Panneerselvam E, Manuel S, Kumar VV, Rai A, eds. Oral and maxillofacial surgery for the clinician. Singapore: Springer; 2021.
- [CrossRef] [Google Scholar]
- Infections of the infratemporal fossa: Imaging/clinical correlations. J Otolaryngol. 1991;20:1-11.
- [Google Scholar]
- Leading causes of facial trauma in the major trauma outcome study. Plast Reconstr Surg. 1995;95:196-197.
- [CrossRef] [PubMed] [Google Scholar]
- Epidemiology of facial trauma. Rev Assoc Med Bras. 2005;51:290-295.
- [CrossRef] [PubMed] [Google Scholar]
- An overview of facial injuries. Surg Clin North Am. 1977;57:987-1010.
- [CrossRef] [PubMed] [Google Scholar]




